
Beyond Heartburn: The Ultimate Guide to Acid Reflux & GERD Management (2025 Edition)
Imagine your stomach is a secure vault, designed to hold potent acid capable of dissolving metal. Now, imagine the lock on that vault is broken. For over 30 years, the medical community’s solution has been to simply remove the acid from the vault, rather than fixing the lock. But in 2025, that narrative is finally changing.
If you are reading this, you likely know the drill: the burning chest pain after a meal, the chalky taste of antacids, and the bottle of Omeprazole on your nightstand that doesn’t seem to work as well as it used to. You are not alone. According to the 2024 update from the National Institutes of Health (NIH) Global Burden of Disease Study, GERD now affects 13.98% of adults globally—that is roughly 1 in 7 people walking around with a fire in their chest.
In my years analyzing health trends and medical breakthroughs, I’ve never seen a shift quite like the one happening right now. We are moving away from the “pop a pill” mentality toward a 360-degree approach that involves cutting-edge drugs, incisionless procedures, and a newfound understanding of how your brain rewires your esophagus.
In this guide, we aren’t just going to tell you to avoid spicy food. We are going to explore the new FDA-approved drug class that works in 30 minutes, the “Silent Reflux” that mimics asthma, and why your sleeping position might be the single most effective tool in your arsenal.
- The New Science: Why PPIs are failing and what PCABs are doing differently.
- The Hidden Link: How anxiety physically alters your esophagus.
- The Fix: From TIF 2.0 procedures to the specific way you need to sleep.
The New Era of Acid Control: PCABs vs. PPIs
For decades, Proton Pump Inhibitors (PPIs) like Omeprazole (Prilosec) and Esomeprazole (Nexium) were the gold standard. They work by blocking the enzyme in your stomach wall that produces acid. But here is the thing: for about 40% of patients, they don’t work well enough, or they stop working entirely.
This is known as “acid breakthrough.” I’ve spoken to countless individuals who take their pill religiously 30 minutes before breakfast, yet still wake up choking on acid at 2 AM. Why? Because PPIs are slow to act and degrade quickly.
Enter Vonoprazan (Voquezna): The 2025 Game Changer
The FDA approval of Voquezna (Vonoprazan) in late 2023 marked the first new mechanism of action for acid reflux in over 30 years. This drug belongs to a class called Potassium-Competitive Acid Blockers (PCABs).
Think of a PPI as putting a slow-drying glue over the acid pump. It takes days to seal fully. A PCAB, on the other hand, is like a cork. It blocks the pump immediately and stays there. According to Colin W. Howden, MD, Professor Emeritus at the University of Tennessee College of Medicine, “The FDA approval of Voquezna provides healthcare providers with a new first-in-class therapeutic option that demonstrated faster healing in the more difficult-to-treat GERD patients.”
| Feature | Traditional PPI (Omeprazole) | New PCAB (Voquezna) |
|---|---|---|
| Time to Full Effect | 3-5 Days | Day 1 (often within 30 mins) |
| Meal Requirement | Must take 30-60 mins before food | Can be taken with or without food |
| Duration | Short half-life | Longer retention in the stomach |
This is revolutionary for patients who struggle with dietary timing or who experience sudden flare-ups that require immediate control.
The “Dementia Risk” Reality Check
You cannot talk about acid reflux medication without addressing the elephant in the room: the headlines linking PPIs to dementia. It’s a terrifying prospect that has led many to quit their medication cold turkey—often resulting in severe esophageal damage.
Let’s look at the actual data. According to a pivotal study published in Neurology in August 2023, researchers found that “Long-term cumulative users of PPIs (more than 4.4 years) had a 33% increased risk of developing dementia.”
My perspective? This data shouldn’t cause panic, but it should cause a pivot. It reinforces why we need to move beyond “pills forever” and look at structural fixes and lifestyle medicine, which we will cover next.
The “Silent” Symptoms: It’s Not Just Heartburn
One of the most common misconceptions I encounter is that if you don’t have burning in your chest, you don’t have reflux. This is dangerous misinformation. Many people suffer from Laryngopharyngeal Reflux (LPR), often called “Silent Reflux.”
Identifying LPR: The Lump in the Throat
In LPR, the acid (and pepsin) travels all the way up the esophagus and spills into the throat and voice box. The tissues here are much more sensitive than the esophagus. You might not feel “heartburn,” but you might experience:
- Globus Sensation: A feeling of a lump or tightness in the throat that won’t go away.
- Chronic Cough: Especially one that worsens at night or after eating.
- Hoarseness: Losing your voice in the morning.
- Post-Nasal Drip: Excess mucus production as the body tries to coat the irritated throat.
Treating LPR requires a different strategy. While standard GERD responds well to acid suppression, LPR often requires a stricter dietary approach (The Acid Watcher Diet) because even weakly acidic foods can activate pepsin molecules lodged in your throat tissue.
The Anxiety-Reflux Loop: Breaking the Cycle
Have you ever noticed your reflux gets worse when you are stressed? For years, doctors dismissed this as patients being “oversensitive.” But in 2024, science confirmed what patients have known all along.
According to a report in Physicians Weekly referencing data from the Gastroenterology journal (Dec 2023), 34.4% of GERD patients suffer from anxiety, with a confirmed bidirectional causal relationship.
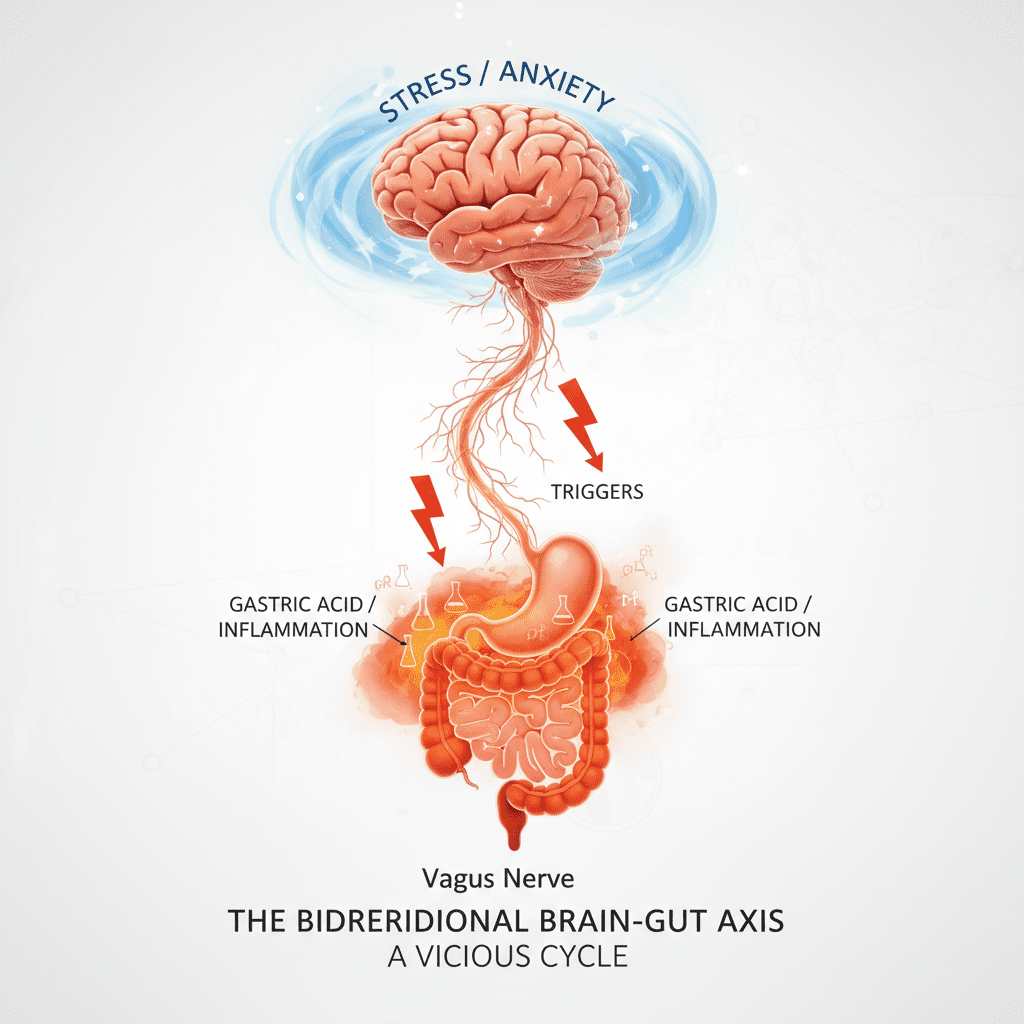
The Vagus Nerve Connection
Here is the physiology: The vagus nerve connects your brain to your gut. When you are anxious, your body enters “fight or flight” mode. This slows down digestion (causing bloating) and actually increases the sensitivity of the esophagus. This means that even a normal amount of acid can feel like a blowtorch.
Conversely, the physical sensation of reflux can trigger a panic response, creating a vicious cycle. Treating the anatomy without treating the mind often leads to failure. I increasingly see gastroenterologists prescribing Cognitive Behavioral Therapy (CBT) or low-dose neuromodulators alongside acid medication to dampen this esophageal hypersensitivity.
Strategic Lifestyle Medicine (Data-Backed)
We’ve all heard “don’t eat chocolate” or “avoid coffee.” While true, these are generic tips. To truly manage GERD in 2025, we need to get specific about physics and chemistry.
The “Left-Side” Sleep Rule
Gravity is your best friend or your worst enemy. If you sleep flat on your back, acid flows freely into your esophagus. But the side you choose matters immensely.
According to Dr. Dang from the Cleveland Clinic (Oct 2024), “Sleeping on the left side makes it harder for acid to reflux up because the stomach looks like a half crescent and acid pools at the bottom.”
When you lie on your right side, the stomach is positioned higher than the esophagus, literally pouring acid into the valve. When you lie on your left side, the stomach hangs below the esophagus, creating a physical trap for the acid. This isn’t just an old wives’ tale; a 2024 systematic review confirmed that left-lateral decubitus positioning significantly reduces nocturnal acid exposure time.
Diet 2.0: pH-Balanced Mediterranean
The days of the bland “boiled chicken and rice” diet are over. That diet is unsustainable and depressing. Current research favors a pH-balanced Mediterranean approach. This involves:
- High Fiber: Fiber helps absorb acid and accelerates gastric emptying.
- Alkaline Waters: Drinking water with a pH > 8.8 can permanently denature pepsin (the stomach enzyme that eats away at your throat).
- Healthy Fats: Olive oil instead of butter. Saturated fats relax the valve; healthy fats are less likely to do so.
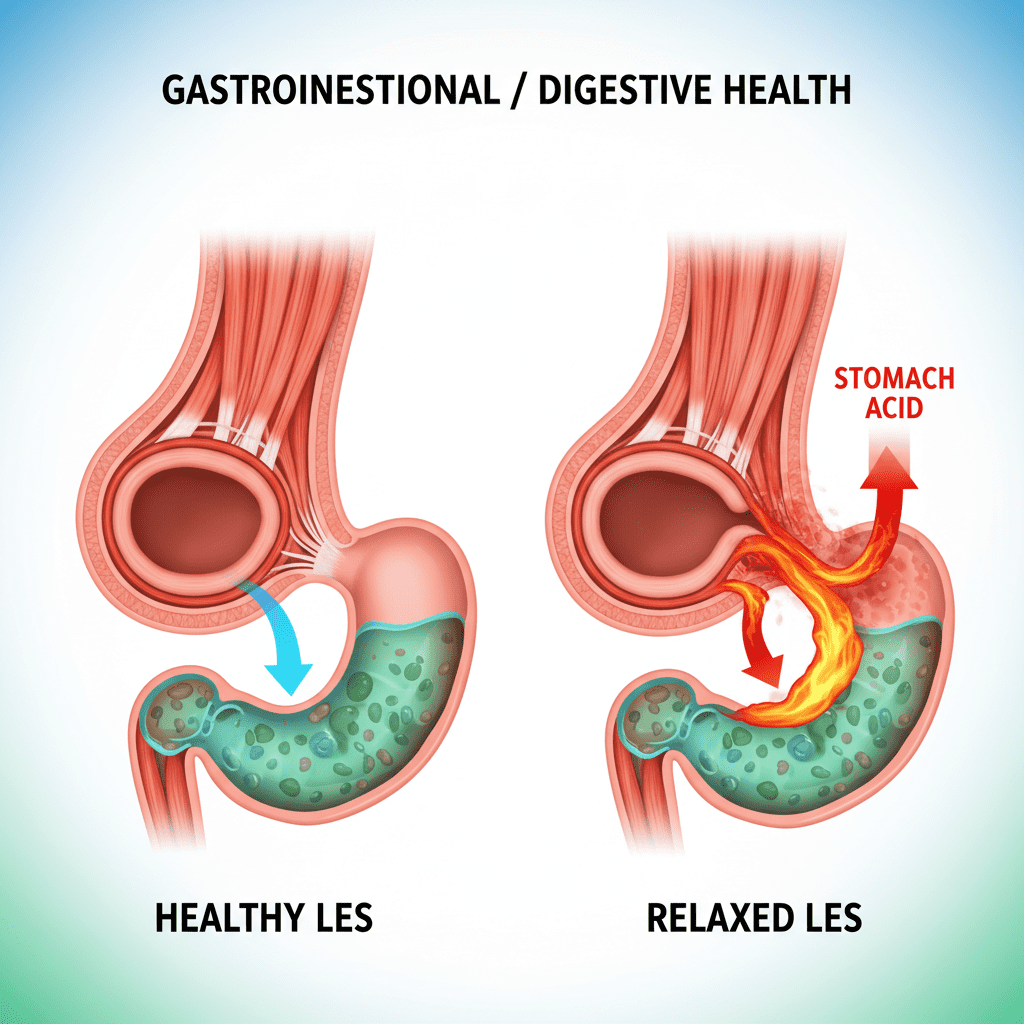
Interventional Solutions: When Pills Aren’t Enough
For some, lifestyle changes and medication simply aren’t enough. The mechanical valve (the Lower Esophageal Sphincter) is too loose. In the past, the only option was the Nissen Fundoplication—a major surgery where they wrap the stomach around the esophagus. It was effective but came with side effects like inability to belch or vomit.
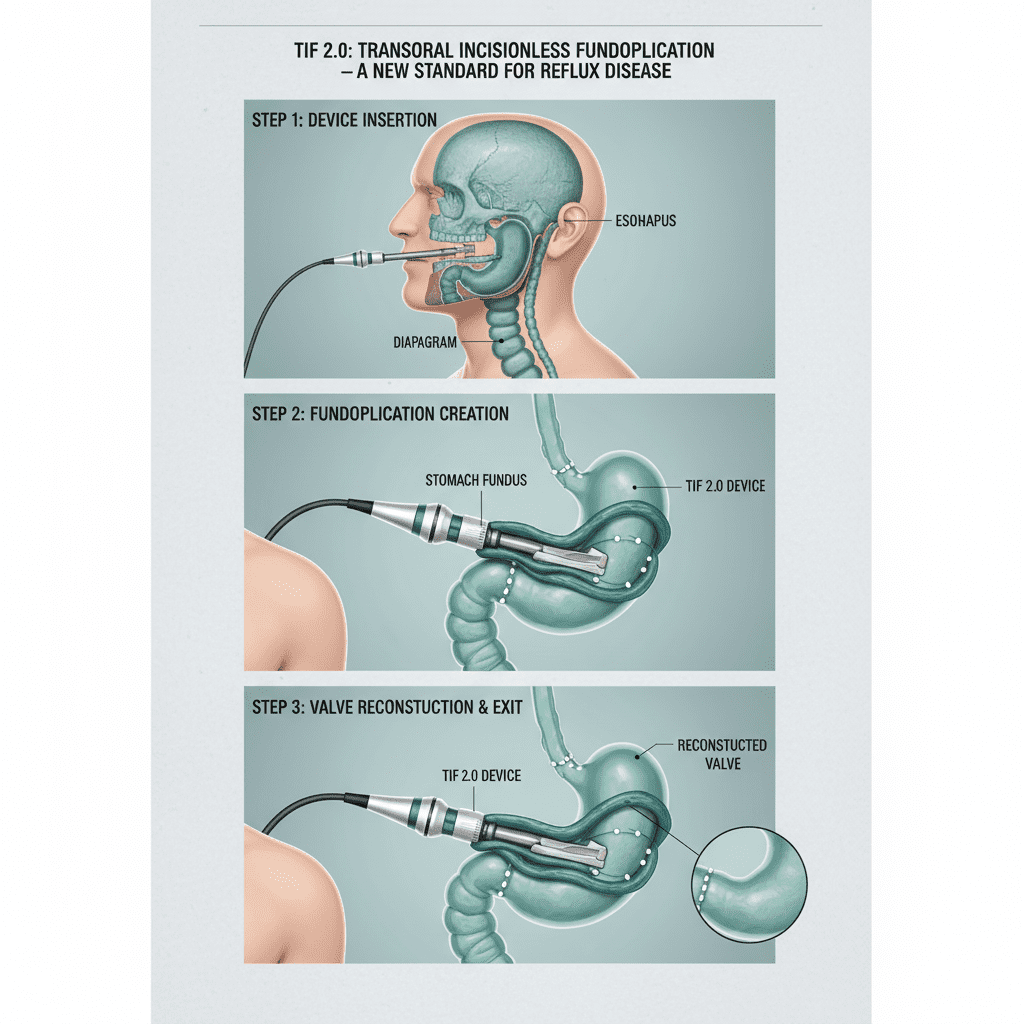
The landscape has changed dramatically with the maturation of the TIF 2.0 (Transoral Incisionless Fundoplication) procedure.
TIF 2.0: No Incisions, High Success
This procedure is performed entirely through the mouth using an endoscope. A device is lowered down the throat to fold and staple the stomach valve tighter, recreating the natural barrier against reflux.
Percentage of patients off daily PPIs after TIF 2.0 procedure (Median 14-month follow-up)
This is particularly effective for those with “Cough-Predominant” GERD. In a 2025 cohort study, researchers found a 63% elimination of atypical symptoms like chronic cough and throat clearing after the TIF procedure. If you have a hiatal hernia smaller than 2cm, this might be the “cure” you have been looking for.
FAQ: Doctor-Approved Answers
- Chew non-mint gum to increase saliva (nature’s antacid).
- Take an alginate-based product (like Gaviscon Advance) to create a foam raft.
- Lie down on your left side only, preferably with your upper body elevated by a wedge pillow.
Conclusion: The Personalized Roadmap to Remission
For too long, GERD patients have been treated as if they are all the same. But your reflux is unique to your anatomy, your chemistry, and your stress levels. The “one-pill-fits-all” era is ending.
If you are struggling, here is my recommended path forward for 2025:
- Evaluate your meds: If PPIs aren’t working, ask your doctor about Voquezna.
- Check your head: If stress triggers your heartburn, treat the anxiety alongside the gut.
- Respect gravity: Commit to left-side sleeping tonight.
- Consider the mechanics: If you are young and don’t want to be on pills for 40 years (risking dementia), consult a specialist about the TIF 2.0 procedure.
You don’t have to live with the fire. With these new strategies, you can finally fix the lock on the vault.